Hospitality Healthscapes: The New Standard for Making Hospitals More Hospitable

By Courtney Suess, Makarand Mody, & Gabrielle Guarracino
What words come to mind when you think of a hospital room? Chances are, your results might sound something like this: Stark. Sterile. Bare. Clinical. These don’t paint a very attractive picture, nor do they engender any comfort for those who find themselves needing to stay at one of these critical institutions. While aesthetics are certainly not the only priority in providing quality medical care to patients, offering a harmonious, customer-oriented model more similar to that embodied in the hospitality industry has been shown to improve patient well-being and influence the willingness to pay higher out-of-pocket expenses in exchange for these services. It’s an intuitive fit, since, after all, the concepts are already very closely linked: both share the same etymological root in the Latin hospes, meaning ‘guest,’ and seek to provide shelter, safety, and succor to those guests, regardless of the circumstances. What might it mean for patients and their overall satisfaction with their hospital stay if the association with the environment shifted to something like: Comforting. Bright. Elegant. Personal? And what specific combination of features would be the most likely to engender that response?
These queries are exactly what our recent study on hospitality healthscapes and patient satisfaction targeted. Using advanced methodology and techniques, such as conjoint analysis and 3D visual representations of hospital rooms, we sought to address the questions: which hotel-like hospital room attributes are most appealing to patients; how do these influence their well-being and willingness to pay higher out-of-pocket expenses; and do these matrices differ based on patients’ health conditions? This study represents the first attempt in the evidence-based design literature to holistically and empirically examine the infusion of hospitality into healthcare by emphasizing the “patient as customer”—and the findings may surprise you.
To better understand our study and research goals, it’s helpful to have some background on the literature and interest in the areas of evidence-based design, the evolving treatment of patients as customers, the concept of a ‘healthscape,’ and more. First—what is evidence-based design, or EBD? This term refers to the focus in research on new types of healthcare facilities that seek to operate very differently from how we think about ‘traditional’ hospitals. EBD draws from a number of areas of study, including the neurosciences, evolutionary biology, psychoneuroimmunology, and environmental psychology, but ultimately, it is “dedicated to the idea that the design of the built environment can enhance the quality of healthcare” (Malkin, 2003, p. 1). Other reviews on EBD also support the idea that the creation of healing environments through the effective design of the physical environment makes hospitals less stressful and promotes faster healing for patients and improved well-being for their families (Dijkstra et al., 2006; Huisman et al., 2012).
The benefits come full circle: while creating this type of healing environment can represent a greater expense for healthcare institutions, it also promotes patient satisfaction, which in turn has the potential to increase the financial bottom line for the institutions. Not only are patients likely to pay more upfront for such services, but leaving their experience more satisfied could also generate positive word-of-mouth feedback and a higher rate of return, should the patient require future medical services. In fact, many hospitals are taking healthcare design to the next level of luxury, competing for wealthy customers who are willing to pay extra and can go just about anywhere. Thus, the changing healthcare landscape presents a strong business case for intelligent EBD decisions—and ultimately, hospitality is a business. Already, many larger healthcare institutions have already started to explore in partnership with the hospitality industry. Even Danny Meyer’s Union Square Hospitality Group has involved itself in this area by teaching hospitals in the New York area how to improve service through its Hospitality Quotient unit.
For healthcare providers who want to create hospitality-inspired environments for their patients, accounting for both patient well-being and revenue considerations, we need to understand design and service features from a customer (patient) perspective. With so many elements that comprise hospitality design and could potentially impact patients’ perceptions of their surroundings with varying levels of importance, hospitals must seek to understand how patients evaluate these elements holistically and empirically. Research has shown that purchasing decisions include the “total product,” with the atmospherics—i.e., physical and controllable environmental components—of the product affecting the buyer’s propensity to consummate a marketing exchange (Kotler, 1973). Similarly, Bitner (1992) used the term ‘servicescapes’ to describe the idea of atmospherics in a service setting. To enable healthcare researchers and providers to understand the dynamics of the total product from a marketing perspective, Hutton and Richardson (1995) developed a theoretical model of healthscapes, which combined Kotler’s atmospherics and Bitner’s servicescapes to measure environmental stimuli, moderators, and responses.
The first component of the healthscapes model includes the environmental dimensions that serve as the stimuli for generating customer responses. These dimensions include the physical environmental aspects and serviceability features that impact the customer experience and create a holistic environment in which customers perceive the servicescape. Perception, in turn, can be influenced by factors such as the service participant’s personality, mood, and demographics, among other things. These moderated perceptions produce a range of multifaceted responses in customers.
Based on the theoretical foundations from the research, we offer a reframed version of the healthscapes model that examines the infusion of hospitality attributes in the healthcare environment (Figure 1). Our framework for understanding hospitality healthscapes includes the underlying components of the Hutton and Richardson (1995) healthscapes model. However, while Hutton and Richardson’s (1995) model also incorporated staff/provider responses, we adopted a narrower definition of the customer as patient alone.
Figure 1. Framework for Hospitality Healthscapes.
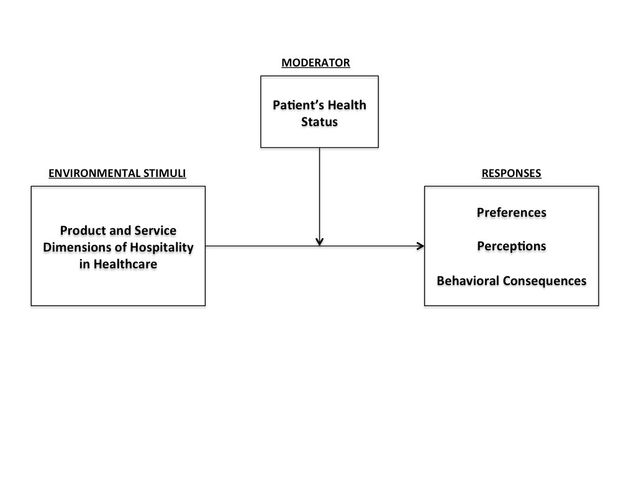 Let’s go through each of these elements individually. The environmental stimuli refers to a multifaceted experience that encompasses not just the physical aspects of the environment, but also but also operations, efficiency, and staff interaction (Kraus and Jensen, 2010). Healthcare providers are not only leveraging design ideas from the hospitality industry, but also the hospitality-style approach of focusing on a service culture. The way these stimuli are perceived could certainly be influenced by an individual patient’s health status, which is the moderating element in this framework. Think about it: doesn’t it make sense that the total package of an environment would matter more to a patient who faces a longer stay in a hospital due to a more prolonged illness? Finally, for the resulting element of ‘patient responses,’ we identified three types of patient responses relevant to testing the application of hospitality features in healthcare: preferences, perceptions, and behavioral consequences. Previously in the literature, patient perceptions of hospitality features in hospital environments hadn’t been measured—which makes our study and our findings truly unique.
Let’s go through each of these elements individually. The environmental stimuli refers to a multifaceted experience that encompasses not just the physical aspects of the environment, but also but also operations, efficiency, and staff interaction (Kraus and Jensen, 2010). Healthcare providers are not only leveraging design ideas from the hospitality industry, but also the hospitality-style approach of focusing on a service culture. The way these stimuli are perceived could certainly be influenced by an individual patient’s health status, which is the moderating element in this framework. Think about it: doesn’t it make sense that the total package of an environment would matter more to a patient who faces a longer stay in a hospital due to a more prolonged illness? Finally, for the resulting element of ‘patient responses,’ we identified three types of patient responses relevant to testing the application of hospitality features in healthcare: preferences, perceptions, and behavioral consequences. Previously in the literature, patient perceptions of hospitality features in hospital environments hadn’t been measured—which makes our study and our findings truly unique.
Procedure
To measure our variables accurately, we used a two-stage procedure to test the hospitality healthscapes model presented in Figure 1. First, we assessed the model for the sample as a whole, i.e., without incorporating the moderating effect of the patient’s health status. We examined patients’ preferences for hotel-like attributes using conjoint analysis, and then assessed their perceived well-being and willingness to pay higher out-of-pocket expenses. Conjoint analysis measures the degree of importance of each product attribute individually, as well as its influence combined with others on the patient’s choice of the overall product (Millar and Baloglu, 2011). Because of the complexity of the inpatient environment, conjoint analysis is an appropriate method and has been used widely to understand preferences in the consumer behavior literature.
In the second stage, we incorporated the moderating effect of the patient’s health status by dividing the overall sample into two groups using cluster analysis: “less healthy” and “more healthy.” We then followed the same procedure as in the first stage. The two-stage procedure allowed us to tease out more nuances pertaining to the hospitality healthscapes model.
Narrowing down the most logical and feasible attributes to measure in the study took careful planning and consultation with a focus group of local hospital physicians. We started with fifteen attributes; but based on their input and our assessment of the “softness,” prevalence, and feasibility of the attributes for both existing and new facilities, a total of nine attributes—each with one upscale hotel-like level and another more cost-effective level, for a total of two levels—were selected. Each of the attributes has been found to impact patient healing and well-being in the literature, so there is theoretical precedent for their inclusion. Figure 2 presents a summary of the measured attributes and their levels.
Figure 2. Selected Hotel-Like Attributes and Attribute Levels.
| Attribute | Level 1 | Level 2 |
| Spa Services | Spa-Quality Bath Amenities (Towels, Soaps/Shampoos, Bathrobe) | In-Room Spa/Salon Services |
| Food and Beverage Services | Kitchenette (Coffee-maker and Refrigerator) | On-Demand Room Service |
| Wall Décor | Artwork | Colorful Walls |
| Luxury Bed Linens | Yes | No |
| Interior Design | Designer-Inspired Furniture | High-end Material Finishes |
| Technology | Hi-Resolution Flat-Screen TV | Smart-Room Technology (Patient Health-Tracking and Entertainment Tablet) |
| Hospitality Services | Concierge Services | Hospitality-Certified Healthcare Staff |
| Aroma/Fragrance | Yes | No |
| Mood Lighting | Yes | No |
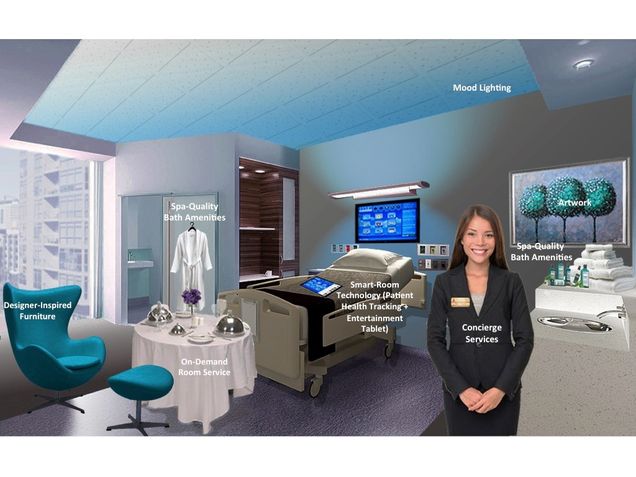
It would have been impossible to ask respondents to rate all scenarios containing all levels of all attributes; a full factorial design would mean 512 scenarios (29). Instead, based on an existing recommendation in the literature that each respondent evaluate a set of profiles two times the number of parameters to be estimated, we presented twenty scenarios to respondents. Respondents were exposed to each of the twenty profiles separately and asked to rate their preference on a scale of 0 (Not at all likely to select) to 10 (Extremely likely to select). To minimize the effects of order bias, the profiles were randomized such that they were evenly presented across the entire sample. Each scenario consisted of a hypothetical hospital room represented as a 3D rendering, incorporating one or the other level of the nine attributes. The use of 3D renderings gave a more realistic sensory portrayal of the attributes and levels, thus enhancing their communicability and capturing a truer reflection of respondents’ preference structures (Hair et al., 2010). Each rendering looked something like the below Figure 3.
Figure 3. 3D Rendering of Sample Hospital Room.
In addition to rating their preference for each of the twenty profiles separately on a scale of 0 (Not at all likely to select) to 10 (Extremely likely to select), respondents—comprised of 406 diverse patients from major metropolitan centers across the United States, all of whom had spent at least one night in a hospital in the previous six months—were also asked questions pertaining to their health status and their perceived well-being from and willingness to pay higher out-of-pocket expenses for a hotel room with hotel-like features. We measured respondents’ health statuses using four variables: the number of times they were hospitalized in the last six months (five response categories: 1, 2, 3, 4, 5 or more), the total number of days for which they were hospitalized in the last six months (five response ranges: 1–5 nights, 6–10 nights, 11–15 nights, 16–19 nights, 20 or more nights), a measure of their perceived (at the time of the survey) physical health, and a measure of their perceived (at the time of the survey) mental health. We used the scales provided by Lin (2014) to measure perceived physical and mental health, with each construct comprising five items measured on a seven-point Likert scale (1 = Strongly disagree to 7 = Strongly agree).
We measured perceived well-being using Tseng and Shen’s (2014) scale, comprising seven items measured on a seven-point Likert scale (1 = Strongly disagree to 7 = Strongly agree). Given the context of the study, i.e., hospitality healthscapes, respondents were asked to indicate their perception of their well-being if they were to stay in a hospital room with hotel-like features. For the constructs of perceived physical health, perceived mental health, and perceived well-being, confirmatory factor analyses were conducted to validate the adherence of the items to their respective constructs, and we averaged the scores for each construct for subsequent analyses. Next, we measured respondents’ willingness to pay using two separate questions adapted from Millar and Baloglu’s (2011) study: their willingness to pay higher out-of-pocket expenses measured on a seven-point Likert scale (1 = Not at all likely to 7 = Extremely likely), and an open-ended question about the percentage that they were willing to pay more. Appendix A lists the exact items that were used to measure the moderator and response variables of the present study.
Results
The results showed that within each pairing level, respondents preferred spa-quality bath amenities in the hospital room over in-room spa/salon services; a kitchenette over more elaborate on-demand room service; artwork over colorful walls; high-end material finishes over designer-inspired furniture; a hi-resolution flat-screen TV over smart-room technology; and hospitality-certified healthcare staff over concierge services. Respondents also indicated a preference for the presence of luxury bed linens, aroma/fragrance, and mood lighting. This offers a more granular look at what specific hospitality offerings yield the greatest satisfaction.
But the relative bigger picture is even more interesting, as we were able to rank the overall importance of the attributes against each other. As the below table illustrates, respondents value the attributes of interior design, hospitality services, and technology the most in their evaluation of a hospital room with hotel-like features.
Figure 4. Relative Attribute Importance Scores.
| Attributes | Importance Score | Rank |
| Spa Services | 11.73 | 5 |
| Food and Beverage Services | 12.16 | 4 |
| Wall Décor | 9.99 | 6 |
| Luxury Bed Linens | 9.20 | 8 |
| Interior Design | 13.93 | 1 |
| Technology | 12.19 | 3 |
| Hospitality Services | 12.95 | 2 |
| Aroma/Fragrance | 8.47 | 9 |
| Mood Lighting | 9.37 | 7 |
Patients perceived higher than average well-being benefits (Mean score = 5.48 > 4, the midpoint of a seven-point Likert scale) if they were to be hospitalized in a room with the hotel-like features offered in the present study. Perhaps even more notably, respondents were largely willing to pay higher out-of-pocket expenses for a hospital room with hotel-like features (Mean score = 4.57 > 4, the midpoint of a seven-point Likert scale). On average, they were willing to pay nearly 38% higher for such rooms. It would appear that respondents would be willing to put their money where their mouths are when it comes to preferences for hotel-like attributes.
These represent the face-value results we garnered from the study. The potential moderating factor of patient health, however, adds an entirely new dimension. Using a cluster analysis, we divided respondents into two groups – “less healthy” and “more healthy” – based on the number and length of hospital visits they reported from the previous six months and their perceived mental and physical health.
The results indicate three significant differences between the preference structures for the two groups. Those who are “less healthy”—i.e., hospitalized more often and for longer durations in the last six months, and in worse perceived physical and mental health—showed a preference for on-demand room service over a kitchenette, versus those who are “more healthy”—i.e., hospitalized less often and for shorter duration in the last six months, and in better perceived physical and mental health—who indicated a preference for a kitchenette. Similarly, the “less healthy” group preferred artwork to colorful walls, while the “more healthy” group picked colorful walls. Finally, those who are “more healthy” derive a significantly higher utility from high-end material finishes than those who are “less healthy.”
The changes didn’t stop there: patient health also influenced the overall ranking of attributes against each other. Once again, several divergences appeared between the ranking tendencies of the two groups. While both still listed interior design as the most important attribute, the “less healthy” group ranked technology far higher than the “more healthy” group, which placed technology as only the fifth most important attribute. Hospitality services had a slight edge in the “more healthy” group, and the ranking of spa services showed an even greater gap between the two groups—ranked third in the “more healthy” group, as opposed to fifth in the “less healthy” group. The table below summarizes the results of the analysis accounting for the moderating influence of patient health, with the major divergences highlighted.
Figure 5. Relative Attribute Importance Scores: Less Healthy vs. More Healthy Patients.
| Attributes | Less Healthy | More Healthy | ||
| Importance Score | Rank | Importance Score | Rank | |
| Spa Services | 11.27 | 5 | 12.28 | 3 |
| Food and Beverage Services | 12.11 | 4 | 12.23 | 4 |
| Wall Décor | 10.43 | 6 | 9.47 | 6 |
| Luxury Bed Linens | 9.15 | 8 | 9.27 | 7 |
| Interior Design | 13.54 | 1 | 14.41 | 1 |
| Technology | 12.52 | 2 | 11.78 | 5 |
| Hospitality Services | 12.39 | 3 | 13.64 | 2 |
| Aroma/Fragrance | 8.49 | 9 | 8.45 | 9 |
| Mood Lighting | 10.11 | 7 | 8.79 | 8 |
And when it comes to financing such amenities, our study showed that—taking health factors into account—the “less healthy” patients would be willing to pay nearly 44% higher out-of-pocket expenses, which is significantly higher than the “more healthy” group (only willing to pay about 31% higher out-of-pocket expenses).
So what does the ideal hospital room look like, taking into account all of this information? It might appear something like this:
Figure 6. Ideal Hospital Room Representing Maximum Utility.

Broader Implications
Moving forward, we hope that different institutions use our healthscapes model, our study, and its results in a number of ways. First of all, we urge researchers to refine and further develop the model by incorporating considerations from the variety of theories that have been applied in traditional hospitality research, from a marketing perspective (Line and Runyan, 2012) and otherwise (Tang, 2014). Now that we have tested the reality that consumers perceive a hospital room in its entirety—as opposed to a bundle of individual attributes—there are myriad empirical opportunities to build on our findings.
But as you might imagine, there are even more practical implications for hospitals to apply our findings to their institutions. Our study clearly indicates patient preferences regarding hospitality features in hospital environments and the potential payoff for the hospitals if they keep these in mind. Interior design consistently comes out on top; but more than just the physical environment, the service atmosphere is also highly desired. Steele et al. (2015) urge departments to provide the necessary resources and training for employees to develop these skills, which lie at the core of the hospitality industry’s experience delivery to its consumers. Armed with an understanding of the communicative power of environmental cues from a patient’s point of view, healthcare providers can strategically plan these cues to correctly communicate the hospital’s image to its customers (Hutton and Richardson, 1995). The themes of comfort, convenience, safety, security, privacy, support, and feeling “at home” can be leveraged in the hospital’s advertising and communication efforts—and the fact that both groups of patients perceived equal well-being benefits from hotel-like hospital rooms alludes to the potential for such communication to attract all types of patients to the facility.
This is an evolving area of study, one that we have barely scratched the surface of. A logical next step involves understanding the preferences and opinions of family and caregivers. With the U.S. serving as a top provider of specialty medical care, it will be fascinating to see how the partnership of hospitality and medical care changes the patient experience and facilitate a more holistic approach to patient care and well-being.

Courtney Raeisinafchi, Ph.D spent 6 years designing and developing hotels and restaurants with Jordan Mozer and Associates, Ltd., an architecture firm based in Chicago, IL, after completing a bachelors degree at the School of the Art Institute of Chicago where she studied architecture. Some notable projects she was involved in includes Marriott’s Renaissance Hotel, Times Square and Hotel 57 in Manhattan, NY; both hotels have received the International Hotel , Motel and Restaurant Society’s Golden Key Awards for Best hotel design. While drafting new proposals for hospitality projects for Jordan Mozer and Associates in Southeast Asia, she began a masters degree, studying hospitality administration, at the University of Nevada, Las Vegas (UNLV) in Singapore. After graduating, she continued to complete her doctoral degree in Hospitality Administration at UNLV in Las Vegas and studied towards a second masters degree in architecture at UNLV’s School of Architecture. Courtney joined the Boston University School of Hospitality Administration in 2013. She teaches the Design and Development Class as well as Lodging Operations and Technology. She is an active quantitative researcher on the topics of hospitality development and built environments, as well as design and atmospherics impacts on consumer behavior.

Makarand Mody, Ph.D. has a varied industry background. He has worked with Hyatt Hotels Corporation in Mumbai as a Trainer and as a Quality Analyst with India’s erstwhile premier airline, Kingfisher Airlines. His most recent experience has been in the market research industry, where he worked as a qualitative research specialist with India’s leading provider of market research and insights, IMRB International. Makarand’s research is based on different aspects of marketing and consumer behavior within the hospitality and tourism industries. He is published in leading journals in the field, including the International Journal of Contemporary Hospitality Management, Tourism Management Perspectives, Tourism Analysis and the International Journal of Tourism Anthropology. His work involves the extensive use of inter and cross-disciplinary perspectives to understand hospitality and tourism phenomena. Makarand also serves as reviewer for several leading journals in the field. In fall 2015, he joined the faculty at the Boston University School of Hospitality Administration (SHA). He received his Ph.D. in Hospitality Management from Purdue University, and also holds a Master’s degree from the University of Strathclyde in Scotland.

17 comments
this is good theses but i don`t clear with your response which is behavioral consequences and i just saw you point only at preference, perception and the moderator. can you explain more about that.
Thanks For Sharing The Very Informative Blog keep it up. Also, Visit the New Technical Blog:- Oxygen Builder Review 2022
Thanks For Sharing The Very Helpful & Informative Article keep it up. Also, Visit:- Magento 2 AJAX add to cart extension
Here are some words that may come to mind when thinking of a hospital room:
Sterile
Clinical
White
Antiseptic
Medical equipment
Bed
Call button
IV drip
Oxygen
Vital signs
Pain
Cambiati Wellness
Illness
Healing
Recovery
Nurses
Doctors
Patients
Family members
Anxiety
Hope
this is good theses but i don`t clear with your response which is behavioral consequences and i just saw you point only at preference, perception and the moderator.
Unfortunately, these descriptions don’t create an appealing image, nor do they promote comfort for individuals who find themselves in need of hospitalization. While aesthetics alone cannot overshadow the importance of quality medical care, adopting a harmonious and customer-oriented model, akin to the hospitality industry, has been proven to enhance patient well-being and even influence their willingness to pay higher out-of-pocket expenses for such services. canadianinsulin.com
His most recent experience has been in the market research industry, where he worked as a qualitative research specialist with India’s leading provider of market research and insights, IMRB International. Chiropractic Townsville
Successful treatment of periodontitis often relies on patient compliance and lifestyle changes. Following the recommended oral care routine, attending regular dental check-ups, and making necessary lifestyle adjustments, such as maintaining a healthy diet and managing stress, can significantly contribute to the effectiveness of treatment. Treating periodontitis
The concept of “Hospitality Healthscapes: The New Standard for Making Hospitals More Hospitable” was a fascinating read, shedding light on the importance of creating a welcoming environment in healthcare settings. As a nursing student in the UK seeking examples for my assignments, this article provided valuable insights into how hospitals can integrate hospitality elements to enhance patient experiences. From designing comforting waiting areas to implementing patient-centered care, the examples mentioned in the article offer practical ideas for improving healthcare delivery. I’m eager to incorporate these concepts into my Nursing assignment examples UK to promote a more compassionate and patient-focused approach to healthcare. Thank you for sharing this informative piece!
The concept of “Hospitality Healthscapes: The New Standard for Making Hospitals More Hospitable” was a fascinating read, shedding light on the importance of creating a welcoming environment in healthcare settings. As a nursing student in the UK seeking examples for my assignments, this article provided valuable insights into how hospitals can integrate hospitality elements to enhance patient experiences. From designing comforting waiting areas to implementing patient-centered care, the examples mentioned in the article offer practical ideas for improving healthcare delivery. I’m eager to incorporate these concepts into my Nursing assignment examples UK to promote a more compassionate and patient-focused approach to healthcare. Thank you for sharing this informative piece!
When most people think of a hospital room, they think of words like stark, sterile, bare, and clinical. These words can evoke feelings of unease, discomfort, and even fear. This is understandable, as hospitals are places where people go to get sick or injured. They are not typically associated with comfort or relaxation.However, there is a growing movement in the healthcare industry to design hospital rooms in a more patient-centered way. cambiati This means creating rooms that are more comfortable, inviting, and home-like. The goal is to make hospitals less intimidating and more conducive to healing.
Your thesis is good, but I’m not sure about your explanation of behavioral consequences. I only noticed you mentioning preferences, perceptions, and the moderator. Port Isaac in Cornwall
I appreciate your insights on the topic. While your points on preference, perception, and the moderator are clear, I’d like more clarification on behavioral consequences. Mental Health Services
Jack in the Box Popcorn Chicken is available in two flavors classic and spicy. You can enjoy it as part of a Popcorn Chicken 50/50 Mix that includes half Classic and half Spicy chicken.
Jack in the Box Popcorn Chicken is available in two flavors classic and spicy. You can enjoy it as part of a Popcorn Chicken 50/50 Mix that includes half Classic and half Spicy chicken.
Jack in the Box Popcorn Chicken
Hospitality Healthscapes revolutionize hospital environments, prioritizing patient comfort and well-being. Integrating soothing aesthetics, efficient layouts, and compassionate care, they redefine the healthcare experience. These spaces alleviate stress, enhance healing, and set a new standard for patient-centered hospitality in medical settings. http://www.heavymug.co