Phacoemulsification
| Manipulate phacoemulsification handpiece | |
| Manipulate second instrument (ie, Seibel chopper, Drysdale, etc) |
|
|
| Phacoemulsification using a divide and conquer technique, using a 0.9mm, 45 degree Kelman tapered ABS tip. |
The mainstay of this surgery, phacoemulsification of the lens using the “phaco” machine can be approached by many different methods. We outline the commonly taught divide and conquer technique which most starting surgeons learn.
Instrumentation
Instrumentation is varied among surgeons, with many newer technologies emerging. Briefly, pump systems between phaco machines vary, from peristaltic to Venturi to hybrid systems. Additional technologies which vary the delivery of phaco energy, such as torsional ultrasound, have also been adapted. The details of these technologies can be sought from phaco textbooks or your instructor, and will not be discussed further here.
Phaco Handpieces and Tips
Typical phaco instrumentation consists of a phaco handpiece (which varies by manufacturer and technology) and a phaco tip (which also varies, as described below). The phaco tip serves to both deliver ultrasound energy and aspirate (ie, vaccum in material) from its open end. Surrounding the phaco tip is the sleeve, which is often of a rubbery consistency. The sleeve allows for irrigation around the tip, lowering the resulting temperature to avoid wound burns. Irrigation typically exits the sleeve from side ports. The sleeve can be adjusted to expose the amount of phaco tip the surgeon desires. Some surgeons prefer to expose a lot of phaco tip, others minimize tip exposure. The sleeve can act as a barrier to tip penetration into lens material. Beginning surgeons are often advised to minimize tip exposure, to provide a higher level of safety. The irrigating ports can also be aligned per the surgeon in reference to the tip. Holding the phaco handpiece such that the phaco tip is bevel up, the irrigation ports on the sleeve are frequently oriented horizontally, such that irrigation is aimed sideways and not directly at the corneal endothelium. Other surgeons angle the irrigating ports at 45 degrees, such that maneuvers that require rotating the bevel can still be accomplished with minimal direct irrigation aimed at the endothelium.
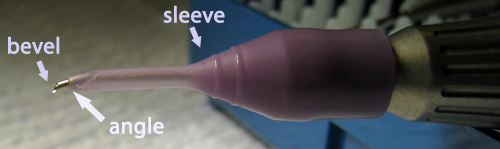
Figure 1: The bevel (here 45 degrees) refers to the very tip of the phaco handpiece. The angulation (here a Kelman style) refers to any bend in the shaft. The sleeve wraps the phaco tip.
There are a variety of phaco tip styles available. Tip angulation refers to the shaft of the tip. Straight tips (or 0 degree), as the name implies, project linearly from the handpiece. Angled tips, such as the Kelman style tips, contain a bend near the end of the tip (usually 22.5 degrees), which can aid in reaching into deep anterior chambers for divide and conquer techniques. These angled tips are also crucial for torsional technologies by providing greater surface area for rotational action.
The bevel of the tip determines the slant at the tip opening. So, a 45 degree tip has a more dramatic slope at the tip opening than a 30 degree tip. This also translates into a larger surface area for a 45 degree tip over a 30 degree tip, making it often preferred for denser lenses. Finally, other modifications to tip design, such as flare (1.1mm tip opening versus 0.9mm tips) which widens the tip opening compared to the tip shaft, can also enhance efficiency. Again, surgeon preference dictates the tip of choice.
Second Instruments, Settings, and Foot Pedal

Figure 2: Typical “sculpt” settings using torsional phacoemulsification (Infiniti phacoemulsification system with Ozil by Alcon Laboratories, Inc, Fort Worth, Texas).

Figure 3: Typical “quad” settings using torsional phacoemulsification (IP mode engaged).
Second instrument designs are also quite varied. Traditional divide and conquer techniques often use a Drysdale manipulator. This instrument has a paddle-like tip to facilitate surface area contact within a groove. Other instruments include choppers, such as the Seibel chopper which we often use. The Seibel has a rounded tip, which avoids bringing any sharp edges potentially near the capsular bag. The Seibel can also serve as a divide and conquer second instrument. The list of choppers is immense, and your instructor can guide you to those available in your operating room.
Settings for phacoemulsification have become somewhat more complex with the advent of torsional ultrasound systems. The roles of torsional energy, traditional coaxial energy, and pulse/burst modes are often intertwined in efficient, modern phaco systems. Example “sculpt” and “quad” settings using torsional phacoemulsification are shown in Figures 2 and 3. A detailed discussion of phaco settings will thus be excluded, and can be discussed with your instructor. However, the principles of 3 primary foot positions remain.
- Foot position 1: Irrigation only. Upon entering the eye, it is vital to maintain irrigation when there is no viscoelastic in the anterior chamber. Failure to do so will allow fluid egress through the open wound and collapse the chamber. Some surgeons prefer “continuous irrigation” such that foot position 1 need not be held to maintain irrigation. This ensures chamber maintenance and less fluctuation in intraocular pressure. This may be beneficial for learning surgeons as well, reducing the need to be as vigilant on maintaining foot position 1 during complex portions of manual activity. Others prefer full control over foot position 1. The setting of the bottle height determines the rate of irrigation.
- Foot position 2: Irrigation and aspiration. In addition to irrigation, aspiration is applied at the phaco tip. This vacuum force allows for lens material to be brought to the tip, and also held there upon occlusion of the tip with material. To emphasize, the flow of material in foot position 2 is towards the phaco tip, so care must be taken to avoid entraping undesirable objects such as iris or capsule.
- Foot position 3: Irrigation, aspiration, and phacoemulsification. As above, the phaco settings will determine in which manner the energy is delivered at the phaco tip. Regardless, foot position 3 should be reserved for the emulsification of lens material, and thus should not be entered unless there is lens material at the tip. Engaging position 3 without lens material can deliver phaco energy to nearby structures, including capsule or iris, resulting in untoward damage. Phaco power can be applied as “fixed” such that a consistent level of energy is maintained throughout foot position 3. “Linear” allows the surgeon to push further down on the pedal to deliver more phaco energy. This behavior is again determined by the surgeon’s settings. Additional modulation of this energy can be applied using pulse and burst modes, as well as newer torsional technologies. Again, consult your instructor or textbook for these advanced topics.
The location of the foot pedals is again surgeon dependent. Most surgeons prefer placing the phaco foot pedal under their right foot, to simulate an automobile foot pedal. The left foot then controls the microscope pedal. Others switch these positions based on preference.
Technique
It is imperative that the surgeon remember a few key points. First, the tip is sharp, and thus any contact with fragile structures such as the iris, lens capsule, or corneal endothelium can be damaging. The utmost care must be given to tip position in the eye. Second, when phaco energy is applied (foot position 3), this energy can be transmitted beyond the tip. Therefore, even proximity and not necessarily contact of the tip with delicate structures can have adverse affects. Again, the utmost care must be given to tip position in the eye.
As stated previously, beginning surgeons often hold phaco instruments too far up the handle. This can result in less control, by translating small hand movements into larger displacements at the instrument tip. For many surgeons, grasping instruments closer to the tip, or “choking up”, can help achieve better control.
Divide and conquer consists of exactly that: divide the lens (grooving and cracking), then conquer through quadrant removal. During the grooving and cracking portion of phaco, aspiration and vacuum settings are low while phaco energy can be modulated as needed based on lens density. These settings are often called “sculpt” settings. During quadrant removal, higher aspiration and vacuum settings are typically desirable to facilitate lens removal with less energy usage.
Divide (Grooving and Cracking)
Phacoemulsification typically begins by inserting the phaco tip into the main wound under irrigation (foot position 1). Note that the sleeve can be easily cut by the phaco tip, so always inspect the sleeve for defects prior to entering the eye. The handpiece may sometimes need to be rotated to fit the phaco tip into the main wound, and rarely an instrument such as a .12 forceps may be needed to assist opening the wound for entry. The non-dominant hand stabilizes the phaco handpiece at the start, as the second instrument often is not needed at this stage. Once in the eye, care must be taken to always maintain irrigation. The previously injected viscoelastic will quickly be evacuated from the chamber once phacoemulsification starts, leaving nothing but irrigation to maintain the chamber.
Some surgeons will proceed to perform a quick cleanup of the anterior cortex which was disrupted during capsulorrhexis. This is accomplished by aspiration (foot position 2), bringing the tip near the material to be evacuated. Doing this step can help improve visualization of the lens, although the initial groove will often automatically result in this cleanup as well.
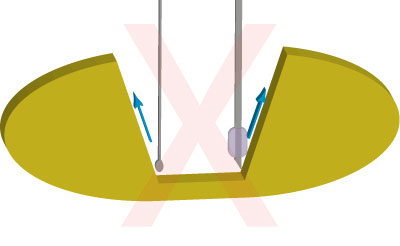
Figure 4: Improperly sculpted groove walls can lead to difficulty in cracking, as instrument tips are unable to maintain proper positioning and can slip along sloped walls (blue arrows).
The first groove in the divide and conquer technique is extremely important. Begin the first groove by orienting the phaco handpiece bevel up. The phaco tip is aimed directly below the wound and brought to the anterior lens surface while the anterior capsule is constantly monitored to ensure it is clear from the tip. Meanwhile, position 3 (phacoemulsification) is engaged. The motion for sculpting follows the lens convex contour. Meaning, the groove starts superficially in the near periphery, dips deeper into the thicker lens center, and then proceeds superficially again at the thinner far periphery. The course of the phaco tip is along a straight line, from under the wound to directly 180 degrees distal to the wound. Phaco power typically is required in greater proportion in the center of the lens, and is gradually decreased as the groove pass reaches the
periphery. For more dense lenses, phaco settings are chosen such that the phaco pedal is “floored” in position 3 while in the center of the groove, and let up towards the periphery. The appropriate groove length is somewhat variable, although we typically aim for the distal
end of the groove to approximate the location of a 6mm capsulorrhexis. If the rhexis is in actuality shorter or longer than 6mm, the groove can be adjusted accordingly. A short groove can sometimes make a distal crack more difficult in soft lenses, which can make quadrants sticky to each other and less mobile during quadrant removal. A long groove risks engagement of the
posterior capsule given the thinner lens periphery. As the distal end of the groove is reached, phaco power is gradually decreased to off. Once the groove pass is completed, be sure to also disengage aspiration as the phaco tip is repositioned for the next pass. The beginning phaco surgeon has a tendency to ride the phaco pedal too long, so be sure to return to irrigation only when the phaco tip is not engaged in lens material.
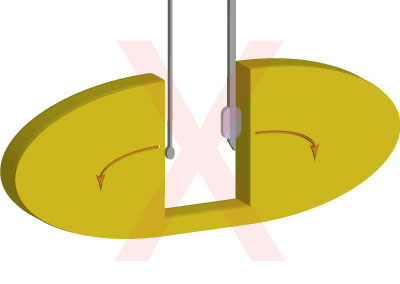
Figure 5: Positioning of instrument tips at inadequate depth can lead to poor delivery of cracking force, and potentially push the posterior plate closer together (red arrows). Such improper cracking can also mash the groove walls making subsequent attempts at cracking more difficult.
The goal is a groove deep enough to allow for an adequate crack. So, successive passes are made, following the lens convex contour until a deep central groove is achieved. An inadequate crack will lead to difficulty in quadrant removal, with pieces unable to be mobilized out of the capsular bag due to residual lenticular attachments. For harder lenses, depth is often not as critical as the lens stiffness allows for easier cracking planes. For softer lenses, however, or so
called “leathery” lens textures, these cracking planes are much more difficult to achieve. Thus, an appropriately deep groove is necessary to allow for a thin posterior lens plate at the base of the groove that will divide easily on cracking manuevers. Excessive attempts to crack a soft lens can often mash the lens, which will essentially bowl out the center of the lens and make further attempts at cracking difficult. Again, an appropriately deep first groove is essential to faciliate cracking maneuvers. Experience will dictate this depth, but generally, as the groove is deepened, the red reflex in the base of the groove will begin to appear. This enhancement of the red reflex
typically indicates a groove deep enough to attempt cracking. Others prefer judging depth against the width of the phaco tip, although varying tip sizes and variation in lens depths can
make this less predictable. Cases where a red reflex is dulled by concomitant disease, such as vitreous hemorrhage, can obscure groove depth judgements. Sometimes, a groove will have uneven depth. In those cases, gentle partial passes can be made at the groove base, to shave off lenticular material in the appropriate areas to ensure a more uniformly deep groove.
The keys to a successful groove include appropriate depth, but also maintaining verticality of the groove walls and ensuring adequate groove width. Sculpting passes must remain linear, to maintain vertical groove walls to allow for easier cracking. Too many stray passes will obliterate the groove wall, leaving no easy surface against which to apply instrument tip cracking force (Figure 4). Likewise, the groove must have enough width to allow for both instruments to reach the base of the groove. We typically like a groove width of 1 1/2 phaco tips. Choose one side of the groove to widen, and carefully sculpt the groove wall. Again, while widening the groove, passes must remain linear in motion to maintain vertical walls.
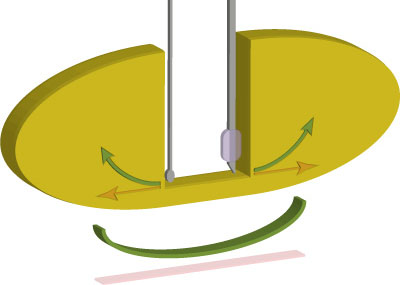
Figure 6: Proper positioning of instrument tips deep in the groove. A horizontal-only displacement of the instrument tips (red arrows) produces only minimal posterior plate displacement (red bar). An “out and up” movement of the instrument tips (green arrows) produces much greater posterior plate displacement (green arc) as well as minimizes zonular stress through avoidance of downward pressure.
Next, the first crack can be made. The entirety of the cracking procedure takes place in foot position 1 (irrigation only). Introduce the second instrument through the paracentesis with the non-dominant hand. Remember, irrigation must be maintained through the phaco handpiece. Positioning both the phaco tip and the second instrument is critical to a successful crack. We typically start cracking attempts centrally. The instruments should be placed such that maximal surface area contact between the instrument and the wall of the groove is achieved. For a second instrument, this often entails pointing the tip vertically to provide a larger contact area against the groove wall. For the phaco handpiece, the bevel can be placed away from the groove wall.
Proceed by placing the instruments deep within the base of the groove against opposing walls. Failure to do so will reduce efficacyand often will mash a soft lens making further cracking attempts difficult (Figure 5). It is often easier to place the phaco tip deep within the groove first, followed by placement of the more petite second instrument tip. Most surgeons leave the groove oriented inline with the main wound, others rotate slightly to improve their angle of approach. Finally, the cracking motion is delivered. The key motion is one of an “out and up” rotational movement of the instrument tips (Figures 6 and 7). The tips should be rotated towards the periphery, and up towards the anterior capsule. This motion will maximize spreading apart of posterior lenticular fibers, and minimize downward zonular force. Simply spreading the instruments apart in the horizontal plane will often not suffice, as the posterior lenticular spread is minimal and wound stretch is problematic. Instead, the motion is one of instrument rotation to move the tips in the proper direction while the instrument shafts remain relatively stable in their respective wounds. In essence, the instruments are “twirled” in the surgeon’s hands. Of note, some surgeons refer a “cross-action” technique, such that the instruments are pushed away against opposing lenticular hemispheres. This technique can be somewhat more difficult to master as the criss-crossing instruments can be easily entangled for beginning surgeons.
A successful crack is indicated by clear separation of the posterior lenticular fibers in the base of the groove. The red reflex will become dramatically apparent. Usually, the crack is started centrally. Once centrally separated, the two instruments can be re-positioned into the peripheral groove and the cracking manuever is repeated. Sequentially, the entirety of the groove can be cracked in this manner creating two completely separated lenticular pieces. Unless the surgeon intends to chop lens material as well, a complete separation should be achieved prior to proceeding if possible.
Figure 7: “Out and up” cracking technique animation.
If the first attempt at cracking is not successful, the process can be repeated. If the process is still not successful, further sculpting is likely indicated to deepen the groove centrally, again looking for enhancement of the red reflex. Once the groove depth is judged adequate, the cracking technique can be repeated.
Once the first crack is completed, or if there is difficulty in obtaining a good first crack, the lens can be rotated 90 degrees to faciliate the next groove. Some surgeons prefer to perform all grooves first, prior to initiating any cracking maneuvers. This can help maintain vertical groove walls with less chance of distortion, facilitating cracking maneuvers.
Rotation can be accomplished by remembering that a tangential force will provide the maximal rotational motion while minimizing zonular stress. Also, as in cracking, the instrument must be placed with maximal surface area in contact with a vertical groove wall. Proceed by placing the second instrument (or phaco tip if preferred) peripheral in the groove. Maximizing surface area contact with the groove wall, apply a tangential force such that the force vector is aimed towards the lens periphery as well as in the direction of desired rotation. Keys to successful rotation are placement of the instrument in the far periphery of the groove to maximize torsion, and applying the appropriate tangential force, that minimizes downward force on the zonules. As stated previously, a good hydrodissection is critical to allow for a freely mobile lens.
Once the lenticular hemispheres is aligned such that the original groove is 90 degrees away from the proposed next groove, quadrants can be created with further sculpting. The same sculpting principles apply as in the primary groove. However, given the changes induced by the original groove, care must be taken as subsequent grooves are shorter in length and typically require far less sculpting as they traverse only one hemisphere. Start against the wall of the hemisphere, sculpting gently to the periphery and maintaining an adequate groove length approximating the edge of a 6mm capsulorrhexis. Again, follow the convex contour of the lens, angling the tip upwards towards the thinner periphery. The appropriate depth can be again judged by the red reflex at the base of the groove. The groove width is also again widened to 1 1/2 phaco tip widths to allow easier cracking.
Once an appropriate groove is achieved, the hemisphere is cracked using the same principles above. Attention is then drawn to the remaining hemisphere. The lens is rotated into position, the groove is sculpted, and the second hemisphere is cracked. When the “divide” portion of the case is completed, the surgeon is left with 4 quadrants. The size of these 4 quadrants often varies, and usually does not matter as long as the pieces are free of attachments.
Conquer (Quadrant Removal)
Shifting to quadrant removal requires adjusting the phaco settings as outlined above (higher aspiration and vacuum settings). The essence of traditional quadrant removal is to engage a quadrant under vacuum, maintain occlusion on the quadrant to allow manipulation of the piece to a safe supracapsular location, and finally phacoemulsify the piece. Phacoemulsification should only be performed when safety of the tip is ensured through proper location of the tip away from capsule/iris/endothelium, and appropriate proximity of desirable lenticular material. Maintaining occlusion prior to phacoemulsification ensures that the phaco tip is in such a safe state. Note that this paradigm is shifting with newer torsional and other technologies that promote alternative phaco energy delivery and intracapsular techniques, however, for the beginning surgeon, we still recommend practicing the utmost safety to prevent untoward complications.
Begin quadrant removal by positioning the quadrant of desire opposite the wound. It may be beneficial to begin by removing a smaller quadrant, and thus rotating the lens fragments to obtain the adequate angle of approach. Smaller quadrants tend to be easier to remove from the bag, and their removal can help create space for subsequent removal of larger pieces. Position the phaco tip such that its opening is against a relatively thicker portion of the quadrant, so there is adequate material behind the tip to protect against perforated completely through the quadrant on phacoemulsification. This is often at the pointed tip of a typical pie-shaped quadrant.
Then, engage foot position 2 (aspiration), attempting to occlude the phaco tip with lenticular material. Other surgeons use the second instrument to tilt the quadrant up to the tip to facilitate occlusion. When occlusion is reached, most phaco machines will emit a high pitched frequency. If occlusion is lacking, a short burst of phaco (foot position 3) may help lodge the tip into the quadrant and achieve occlusion. Once occlusion is reached, it is vitally important to maintain this level of aspiration only. Decreasing aspiration (letting up on the pedal) will release occlusion while phacoemulsifying further (stepping further on the pedal) could potentially emulsify through the lens and engage capsule. If occlusion is lost, the above steps should be repeated to re-engage the quadrant prior to proceeding.
Once occlusion is achieved and maintained, the quadrant will be under the surgeon’s control, and can be manipulated and positioned as the surgeon sees fit. The quadrant is thus pulled centrally and lifted up out of the bag. The pupillary plane or near supra-pupillary plane is typically a safe location to proceed with more vigorous phacoemulsification of the piece. Previously placed viscoelastic will protect the endothelium, and often the second instrument can be used to gently hold back the remaining quadrants and capsule. Phaco proceeds as long as the tip is occluded or material is easily aspirated into the port. Phaco energy should not be delivered once the quadrant is disengaged or further phaco does not result in further emulsification of the lens. In other words, if nothing is happening at the tip while in position 3, position 3 should be immediately disengaged to avoid further energy delivery and potentially undesirable collateral damage. The repeated in and out of position 3 is continued until the quadrant is completely emulsified.

Figure 8: Typical “epinuclear” settings using torsional phacoemulsification.
During quadrant removal, the second instrument can help in a variety of ways. For one, it can be used to manipulate lenticular pieces to bring them in proximity of the phaco tip. Care must be taken to not phaco the second instrument tip however, as this can create sharp edges or points on the tip which make it more dangerous near the capsule. The second instrument can also be used to tamponade remaining lenticular quadrants or capsule. While second instruments designed to be rounded and safe near the capsule can sometimes contact the capsule without damaging it, as above, inadvertent creation of sharp edges on even rounded instrument tips can be problematic and thus contact with the capsule should be minimized even with these instruments. Other uses of the second instrument include quadrant rotation, and iris tamponade or manipulation to prevent incarceration.
To complete quadrant removal, the remaining quadrants are rotated into position and emulsified using the principles above. Care must be taken when the last quadrant is approached, as the lack of remaining lenticular material can make the posterior capsule more likely rise anteriorly with anterior chamber pressure fluctuations making it more likely to be engaged by the phaco tip.
Quadrants particularly difficult to lift out of the bag can be approached by a few methods. If the quadrants are not completely cracked, further attempts to crack can be very beneficial in creating more mobile pieces. Otherwise, viscoelastic can be introduced to “float” the pieces up into the pupillary plane. Clearly, haphazardly maneuvering the phaco tip into the peripheral capsular bag attempting to engage lenticular material will often result in capsular rupture. Again, maintaining a safe, central location of the phaco tip will go far in reducing capsular complications for the beginning surgeon.
Any remaining epinuclear bowl can be carefully removed using lowered phaco energy and vacuum settings (Figure 8). However, it may be safer for the beginning surgeon to use I&A for epinuclear removal, see the “I&A” section for more details.