Irrigation and Aspiration
| Manipulate I&A handpiece | |
| Stabilize dominant hand |
|
|
| Irrigation and aspiration using steel sleeved handpiece and 45 degree tip. |
Irrigation and aspiration (I&A) cannot be overlooked as a critical step in phacoemulsification, as inattentive I&A can lead to capsular rupture. Following basic principles and techniques will help avoid such complications.
Cortex exhibits a high degree of “followability,” as cortical material flows to the I&A tip easily allowing for aspiration without difficulty. The same is not true of more solid, stiff nuclear material. Cortex is encountered in two layers:
- Epinucleus, or supranuclear cortex, refers to the soft, continuous region of cortex surrounding the nucleus. Hydrodelineation can produce an epinuclear shell that can be removed as a single bowl.
- Peripheral cortex, as the name implies, is located beneath the anterior capsule, into the equatorial region, and lining the posterior capsule. Peripheral cortex tends to have a more fibrous texture with firm attachments at the equator and anterior capsule which are not present along the posterior capsule. Therefore, aspiration of peripheral cortex requires a stripping action from the equatorial and anterior lens capsule in order to achieve a meticulous cortical cleanup.
Instrumentation

Figure 1: Left to right: 45 degree tip, straight tip, and 90 degree tip.
There are a variety of I&A handpieces and tips available (Figure 1). Coaxial (ie, irrigation and aspiration ports located on a single handpiece) and bimanual (ie, irrigation and aspiration ports are on separate handpieces) setups can be used. The handpiece sleeve itself can be composed of metal, or newer silicone soft sleeves which provide better wound sealing and more stable anterior chamber maintenance. Since the I&A handpiece is generally thinner than the phaco handpiece, a well constructed main wound is crucial to minimize the efflux of fluid around a metal handpiece. Finally, the tip can be straight or angled, up to 90 degrees for more facile subinicisional cortex removal. Other tips have roughened surfaces or are made from silicone to allow for posterior capsular polishing. We typically use a steel, coaxial, side-ported aspiration 0.3mm orifice handpiece with a 45 degree tip.
Foot Pedal and Settings
There are two foot positions in I&A mode:
- Foot position 1: Irrigation only. As in the phaco step, maintaining irrigation is critical to avoid chamber collapse. Some surgeons again prefer continuous irrigation.
- Foot position 2: Irrigation and aspiration. In addition to irrigation, aspiration is applied at the I&A tip. Aspiration can be applied as “fixed” so that vacuum will rise to a fixed level regardless of how far down into position 2 the surgeon steps. “Linear” aspiration allows the surgeon control the amount of aspiration by the depth of foot pedal travel. Again, the surgeon can control this behavior through the phaco machine settings.
| Cortical Removal | Capsular Vacuum | Viscoelastic Removal | |
| Aspiration (ml) | 40 | 10 | 50 |
| Vacuum (mm Hg) | 500 | 10 | 500 |
| Bottle Height (cm) | 100 | 100 | 100 |
Table 1: Settings for I&A in various situations. |
|||
Most surgeons adapt their I&A settings based on personal and situational preference (Table 1). High vacuum settings allow for ease in epinuclear removal and cortical stripping. Capsular vacuum demands much lower vacuum and aspiration rates. While capsule may still be incarcerated at these low settings, the safety margin is greatly enhanced when working near the posterior capsule in this mode. Removal of viscoelastic requires adequate irrigation of the anterior chamber, which can be performed under both high vacuum and aspiration rate settings.
Technique
Epinucleus and Nuclear Chips
Following phacoemulsification of the nucleus, a residual epinuclear bowl may sometimes remain. Using the I&A handpiece, this epinuclear shell can be gently relieved from its capsular attachments by approaching the sub-anterior capsule rim with the I&A aspirating port facing up, and applying gentle aspiration until occlusion is achieved. The cortical material is then pulled towards the pupillary center and released. This procedure is repeated for the entire circumference of the epinucleus, attempting not to aspirate any epinucleus at this point. The maintained epinuclear rim can be used as a protective shell against capsular entrapment in the I&A port. Once the epinucleus is completely free, it can be brought into the anterior chamber for aspiration, or, the I&A tip can be brought underneath the bowl with the aspirating tip up to allow for safe removal.
Occasionally, small nuclear remnants are left following phacoemulsification which are often too stiff to be aspirated using the I&A alone. A second instrument can be inserted through the paracentesis, and used to “mash” the material into the I&A side port once occlusion is achieved.
Cortical Stripping
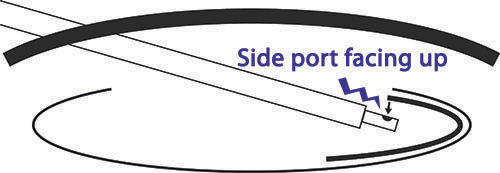
Figure 2: A straight I&A tip with port facing up for cortical removal.
Peripheral cortical fibers may be present as interspersed wisps or as confluent cortex, and require a cortical stripping technique to ensure their removal. To reach peripheral cortex to the left of the incision, the handpiece should be positioned along the right edge of the wound. The reverse position at the left of the wound is employed to reach cortex to the right of the incision. Some surgeons prefer to remove the more challenging subincisional cortex first, while others save subincisional cortical cleanup until the end.
Introducing the I&A tip into the AC with the side-port facing up, the sub-anterior capsular region is approached (Figure 2). Care must be taken to maintain distance from the posterior capsule as well as the anterior capsule edge. Gentle aspiration is then applied to engage cortical fibers. If occlusion is not reached or inadequate quantity of cortex is grasped, the tip can be re-introduced under the anterior capsule, and towards the equator if necessary. Once the port is full of cortical material, occlusion will be achieved with a rise in vacuum. The tip is withdrawn towards the pupil, maintaining occlusion through continued aspiration. As the anterior capsular edge is cleared, more vigorous aspiration can be applied, allowing the I&A vacuum to continue stripping the cortical fibers. Alternatively, with cortical material filling the port, manual stripping of the cortex can be performed with gentle rotation of the tip towards the pupillary center, followed by aspiration once the cortex is free of attachments. This rotational technique can be very helpful with subincisional cortex (Figure 3).
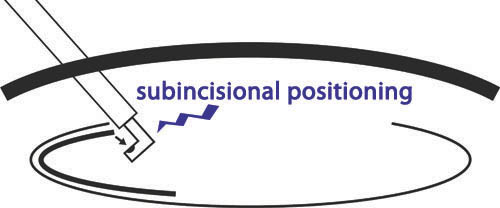
Figure 3: A 90 degree I&A tip rotated for subincisional cortex removal. To ensure safety, the tip should be rotated towards the center of the pupil, port up prior to vigorous aspiration (see video for demonstration).
This technique is repeated for the full circumference of the capsular bag. In order for I&A assisted cortical stripping to be successful, proper occlusion with cortical material is necessary. Often, large portions of cortex can be incorporated by repeated engagement of the sub-anterior capsular cortical fibers in a sweeping arc.
Capsular Vacuum
Sometimes, a resilient posterior cortical plaque may persist. First, to reduce the likelihood of posterior capsular rupture, the I&A settings should be adjusted for capsular vacuuming (Table 1), reducing vacuum and aspiration rate for greater safety near the capsule. The I&A tip can then be brought with the side port perpendicular to, or carefully facing down towards, the posterior cortical material (Figure 4). A gentle sweeping motion can be used to catch the edge of the plaque, and pry the fibers from the capsule. A studded tip may be used to provide greater friction against the fibrotic cortical fibers. If an edge can be lifted, viscoelastic may also be injected under this edge to help “visco-dissect” the plaque.

Figure 4: Technique for capsular vacuuming, first ensuring that the I&A settings have been appropriately adjusted.
Caution must be exercised in removing resilient posterior capsular plaques, such as those found in small posterior polar cataracts. In this situation, an irregularity in the posterior capsule may be pre-existing, or easily induced, and may lead to vitreous presentation. In such cases, it may be prudent to leave the cortex for later neodymium-doped yttrium-aluminum-garnet (nd:YAG) laser capsulotomy.