Avoiding the Public Health Triple Fail.
 As we reflect on Martin Luther King Jr. Day this weekend, we rerun a previous Dean’s Note, on social justice and public health, in this week’s SPH This Week. Today, I wanted to talk about a concept I have been mulling recently: How we avoid making mistakes in public health.
As we reflect on Martin Luther King Jr. Day this weekend, we rerun a previous Dean’s Note, on social justice and public health, in this week’s SPH This Week. Today, I wanted to talk about a concept I have been mulling recently: How we avoid making mistakes in public health.
The triple aim in health care was articulated by the Institute for Healthcare Improvement as a framework to facilitate the advancement of health system performance in the United States. This triple aim includes “improving the individual experience of care; improving the health of populations; and reducing the per capita costs of care for populations.” In other words, the triple aim aspires to the delivery of care that is efficient, associated with patient satisfaction, and cost effective. By contrast, a triple fail refers to a situation in which no single element of the triple aim is met. Triple-fail events are thus health events characterized by inefficient interventions with low patient satisfaction and low cost-effectiveness. Accordingly, while the triple aim serves well as an aspirational goal, the triple fail indicates a clear benchmark for events to be avoided at all costs. Today, a note about two scenarios in contemporary public health that we might consider to be triple fails, both by way of learning from what we are not doing well, and anticipating where we might improve in the future.
We take as examples of triple fail scenarios in public health, (1) pharmaceutical approaches to chronic non-cancer pain and the opioid epidemic, and (2) a misdirected focus on personal risk factors in the obesity epidemic.
Chronic Pain and the Opioid Epidemic
Pain (including chronic and acute pain, cancer and non-cancer pain) is a serious problem worthy of the attention of the public health and medical communities. Unfortunately, our approach to dealing with undertreated pain over the past two decades has contributed directly to what is now a rampant epidemic. In the last 20 years, prescription opioids have been dispensed in great numbers to treat chronic non-cancer pain, and, as reflected in Figure 1, an epidemic of overdose has followed as an unintended and powerful consequence. The causes of this over-prescription range from the well-intentioned efforts of physicians to address a real patient problem to systematic attempts by pharmaceutical companies to increase sales of powerful opioid analgesics. Regardless of the etiology, it is now abundantly clear that our approach to one problem has created another, potentially bigger, problem. Importantly, it is not at all clear that the problem that the increased use of opioids intended to solve—pain—was actually improved at all through the prescription of opioids. A systematic review that examined the effectiveness of opioids in the treatment of chronic non-cancer pain evaluated 111 randomized controlled trials and found there to be fair evidence for the treatment of osteoarthritis with Tramadol, and poor evidence for all other medications and conditions. Few studies followed up beyond 12 weeks of treatment. In addition, patient satisfaction among patients treated with opioids appears low, as shown in surveys of side effects and satisfaction among patients taking Oxycodone and Hydrocodone. Given the high potential for opioid misuse, patient satisfaction, even if improved with the use of opioids, is clearly in conflict with safe practice. This, coupled with the evidence that there is a clear net cost to patients and society through the increased use of opioids, makes the opioid epidemic an example of a public health triple fail, i.e. an effort to deal with a problem that was tackled with an ineffective intervention, with low patient satisfaction and low cost effectiveness.
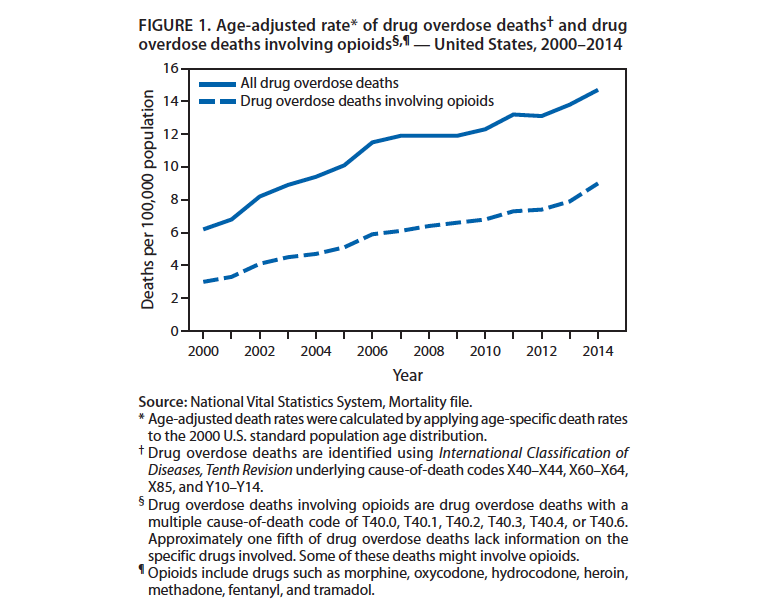
Russ RA, Aleshire N, Zibbell JE, Gladden RM. Increases in drug and opioid overdose deaths–United States, 2000—2014. MMWR Morb Mortal Wkly Rep. 2016; 64: 1—5; http://www.ncbi.nlm.nih.gov/pubmed/26720857
The Obesity Epidemic—A Misplaced Focus on Individual Risk Factors
The obesity epidemic emerged at an alarming pace in the US in the 1980s, with more than a doubling of the prevalence of obesity in the country over two decades. As shown in Figure 2, as of 2015, there are no US states with less than a 20 percent prevalence of obesity, an extraordinarily different picture than the one that existed merely 20 years ago. There is abundant evidence that obesity is associated with increased risk for a number of health problems, including hypertension, type 2 diabetes, coronary heart disease, some cancers, and osteoarthritis, among many other conditions. The question then for us collectively has been: How do we deal with the rapidly unfolding obesity epidemic? Unfortunately, the dominant approaches to tackling obesity have principally focused on lifestyle treatments involving diet and exercise, despite the evidence that these approaches likely do relatively little to reduce obesity. A review of reviews found that interventions to reduce obesity through diet and physical activity yielded generally modest outcomes. Further, a review that examined long-term maintenance of weight-loss outcomes found small benefits. Interestingly, a recent study examined augmentation of behavioral treatment of weight loss with a wearable activity-monitoring device (similar to a fitbit), only to find that at 24 months those who wore the monitor had lost less weight (mean 3.5 kg) than the control group (mean 5.9 kg).
This struggle to keep weight off is reflected clearly even in population culture, including recently among former contestants from the weight loss competition reality television show “The Biggest Loser.” Echoing the sentiments of those former contestants, a study of obese college students attending a university weight loss clinic found that they were disappointed by the standard weight loss outcomes produced by best practice behavioral treatments. Regarding the cost effectiveness of diet and exercise interventions, scientific literature has been mixed. The ACE study found that treatments involving counseling to induce behavior change related to diet and physical activity are not very cost-effective, while other studies have suggested some potential for cost effectiveness, even as the lack of evidence for the efficacy of these approaches makes these claims dubious.
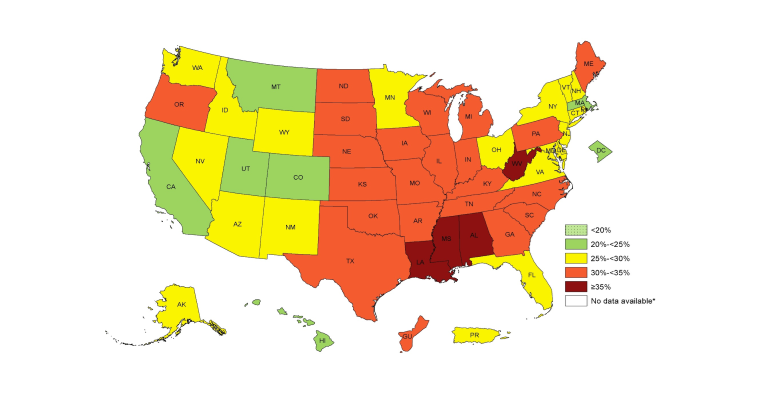
Figure 2. Prevalence of Self-Reported Obesity Among US Adults by State and Territory, BRFSS, 2015
Adult Obesity Prevalence Maps. Centers for Disease Control and Prevention Web Site. https://www.cdc.gov/obesity/data/prevalence-maps.html Accessed January 11, 2017.
Avoiding Future Public Health Triple Fails
The recent opioid and obesity epidemics strike me as good illustrations of public health triple fails, i.e. inefficient approaches that make few of us happy, with, unsurprisingly, low cost effectiveness. It is then critical for us to ask: Why did this happen? Why did we take these approaches to begin with? Our approach to pain was driven perhaps by good intentions, but also by clear initiatives by actors with particular self-interest to push forward one very specific solution (i.e., to increase opioid prescribing) that turns out to have been the wrong strategy. Our approach to the obesity epidemic falls in line with an overwhelming cultural narrative around the power of individual self-improvement, ignoring the large body of evidence about obesogenic environments, and obviating the potential role of structural efforts to create contexts where healthier food is more available, opportunities for exercise are more abundant, and where nutrient-poor, calorie-rich beverages and foods are harder to come by. Unfortunately, these failures have real consequences, in deaths that would otherwise have been preventable, and in lives lived much less fully, burdened by disease. These examples illustrate well the perils involved in population shifts, and the need to carefully weigh approaches, anticipating potential negative consequences. This is in no small part why I have been a skeptic about some proposed public health approaches where I feel the evidence has been lacking. Of course, skepticism is easy. Action is much harder. Perhaps a recognition of our historic failures can help to ensure we do not repeat them in the future, even as we boldly embrace efforts to improve population health.
I hope everyone has a terrific week. Until next week.
Warm regards,
Sandro
Sandro Galea, MD, DrPH
Dean and Professor, Boston University School of Public Health
Twitter: @sandrogalea
Acknowledgement: I am grateful for the contributions of Greg Cohen, MSW, to this Dean’s Note.
Previous Dean’s Notes are archived at: https://www.bu.edu/sph/tag/deans-note/
Comments & Discussion
Boston University moderates comments to facilitate an informed, substantive, civil conversation. Abusive, profane, self-promotional, misleading, incoherent or off-topic comments will be rejected. Moderators are staffed during regular business hours (EST) and can only accept comments written in English. Statistics or facts must include a citation or a link to the citation.