Population Health Is Key to Creating a Safe, Secure Country.
 The United States prioritizes national security. We express this priority in a number of areas, from the money we spend on defense, to our political rhetoric, to our foreign policy. The Trump administration’s recently released “skinny budget” reinforces our focus on security. Characterized as a “hard power budget,” it allocates an additional $54 billion for defense spending, while cutting many social programs that promote population health. This budget is problematic in a number of ways; centrally, it seems to suggest that we can create a safer nation by investing heavily in defense at the expense of initiatives that safeguard well-being and improve the conditions of health. Trump’s budget may ultimately only carry symbolic weight, as a reflection of this new administration’s values and goals—it is unlikely to be approved by Congress in its present form. However, the values it represents are undeniably shared by many in a country where we frequently view national security from a combative, military perspective. I would argue that this view is simply wrong; that without building a healthier nation, the US is far from being secure, and that it is an oversight to think that we can create a country that is simultaneously safer and less healthy. I had the privilege this week of being a part of a National Academy of Medicine meeting, as part of the Academies’ Health Security portfolio of work, pushing me to think a bit about this, and writing here a note on population health as a security imperative, and how we can improve our security through a focus on the foundational conditions of health.
The United States prioritizes national security. We express this priority in a number of areas, from the money we spend on defense, to our political rhetoric, to our foreign policy. The Trump administration’s recently released “skinny budget” reinforces our focus on security. Characterized as a “hard power budget,” it allocates an additional $54 billion for defense spending, while cutting many social programs that promote population health. This budget is problematic in a number of ways; centrally, it seems to suggest that we can create a safer nation by investing heavily in defense at the expense of initiatives that safeguard well-being and improve the conditions of health. Trump’s budget may ultimately only carry symbolic weight, as a reflection of this new administration’s values and goals—it is unlikely to be approved by Congress in its present form. However, the values it represents are undeniably shared by many in a country where we frequently view national security from a combative, military perspective. I would argue that this view is simply wrong; that without building a healthier nation, the US is far from being secure, and that it is an oversight to think that we can create a country that is simultaneously safer and less healthy. I had the privilege this week of being a part of a National Academy of Medicine meeting, as part of the Academies’ Health Security portfolio of work, pushing me to think a bit about this, and writing here a note on population health as a security imperative, and how we can improve our security through a focus on the foundational conditions of health.
Public health’s national security role is often narrowly defined as a means of defending against threats, such as bioterrorism and infectious disease outbreaks. While these functions are indeed key, public health is also linked to national security in more fundamental ways, through its concern for the structural forces that undergird a society’s stability and health. This concern dovetails with the priorities of national security; i.e., to guard against threats to the social, political, economic, and environmental stability of a given country or region. Identifying these threats, and distinguishing them from those that are tangential to core social structures, are critical imperatives for both national security and public health. The longstanding problem of HIV/AIDS in sub-Saharan Africa is an example of such a threat; one that challenges not only the health, but the very stability of the region it affects. This instability is caused by a number of factors, including the loss of public servants, an orphan crisis, and food insecurity—all precipitated by the AIDS crisis (Figure 1).
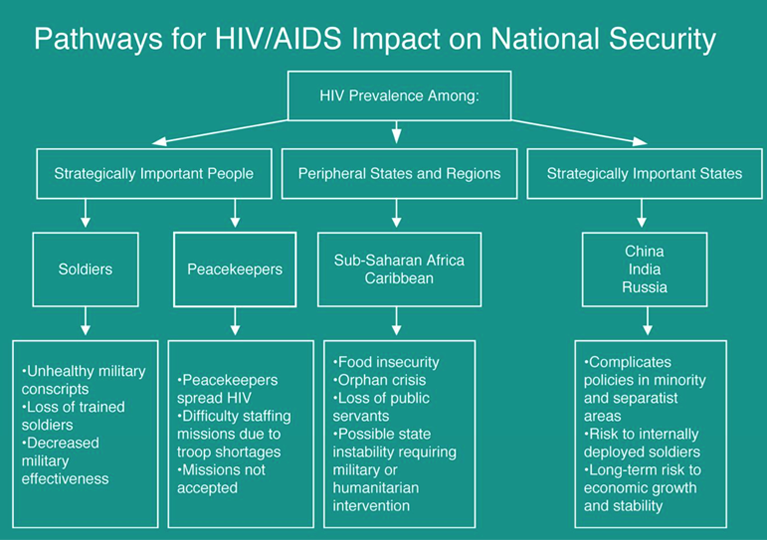
Feldbaum H, Lee K, Patel P. The National Security Implications of HIV/AIDS. PLOS Medicine. 2006; 3(6): e171. doi: 10.1371/journal.pmed.0030171
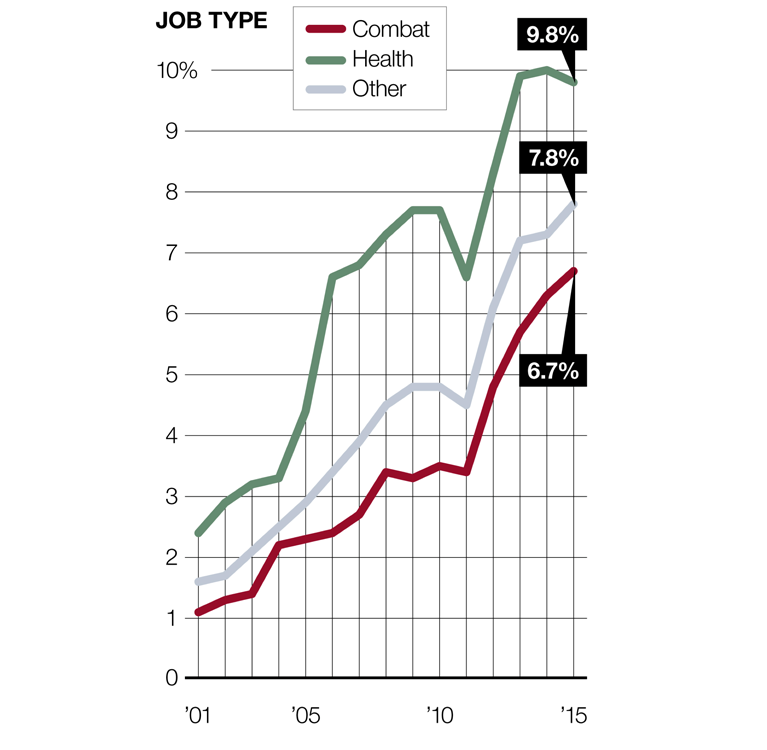
How do health risks, then, pose a security threat to the US? In this country, by way of example, obesity clearly represents such a threat, putting pressure on our health system and our economy, and undermining our well-being. Obesity rates are rising in the US, costing us an estimated $147 billion to $210 billion per year in healthcare spending. In 2015, obesity rates among adults exceeded 35 percent in four states, contributing to the burden of associated conditions such as heart disease, diabetes, and infant mortality. Obesity also deepens health divides, fueling gaps in well-being that exist between vulnerable minority groups. Between 2011 and 2012, for example, the overall obesity rate in the US was 34.9 percent. During this period, adult obesity rates were highest in the black community, at 47.8 percent, and the Latino community, at 42.5 percent, significantly higher than the 32.6 percent obesity rate for whites. Another vulnerable population, whose struggle with obesity is not incidental to our national security, is the US military. The percentage of military personnel classified as overweight has increased significantly since 2001. Close to 8 percent of the military’s active-duty force is now classified as clinically overweight, compared to 1.6 percent in 2001 (Figure 2).

Tilghman A. The US military has a huge problem with obesity and it’s only getting worse. Military Times. September 11, 2016. http://www.militarytimes.com/articles/the-us-military-has-a-huge-problem-with-obesity-and-its-only-getting-worse Accessed March 8, 2017.
This trend even extends to combat troops. While combat troops remain less likely to be overweight than the overall force, today about 1 in 15 service members assigned to combat arms career fields are flagged for being overweight (Figure 3). This is a marked increase from 2001, when about 1 in 100 combat service members were flagged.
Tilghman A. The US military has a huge problem with obesity and it’s only getting worse. Military Times. September 11, 2016. http://www.militarytimes.com/articles/the-us-military-has-a-huge-problem-with-obesity-and-its-only-getting-worse Accessed March 8, 2017.
While changes in military training and diet may partly account for this problem, it is hard not to see rising military obesity rates as part of the larger issue of obesity in the US, with 20 percent of male military recruits and 40 percent of female recruits classified as initially too overweight to join the ranks. While many in the media have called military obesity a national security threat largely because of its potential effect on the combat readiness of service personnel, obesity among the armed forces is actually representative of an even greater security threat presented by obesity—its broader role in making Americans less healthy at all levels of society.
The divide between the view that national security is embodied by our military might and the view that national security begins with building a healthier society is well reflected by the Trump budget. With its deep cuts to the Environmental Protection Agency, the National Institutes of Health, and the Department of Housing and Urban Development, the budget has raised the question of how we, as a society, define national security. Fundamentally, a healthy nation is a secure nation. No matter how powerful our military is, we cannot be truly secure unless we invest in mitigating problems like the health gaps, chronic disease, and opioid abuse that currently undermine the health of so many Americans. If left unattended, these problems stand to deepen inequality, burden our health system, strain our economy, and threaten the foundations on which we have built our social and civic life. If we appreciate that health is a security imperative, then investing in improving the social, economic, and environmental conditions of health is an extension of this imperative, and constitutes a public good. Just as we have shown a willingness to spare no expense on our defense, our commitment to public health should be no less well-resourced, if we are to maintain the programs that truly keep us healthy and our nation secure.
I hope everyone has a terrific week. Until next week.
Warm regards,
Sandro
Sandro Galea, MD, DrPH
Dean and Robert A. Knox Professor
Boston University School of Public Health
Twitter: @sandrogalea
Acknowledgement: I am grateful to Eric DelGizzo for his contribution to this Dean’s Note.
Previous Dean’s Notes are archived at: https://www.bu.edu/sph/tag/deans-note/
Comments & Discussion
Boston University moderates comments to facilitate an informed, substantive, civil conversation. Abusive, profane, self-promotional, misleading, incoherent or off-topic comments will be rejected. Moderators are staffed during regular business hours (EST) and can only accept comments written in English. Statistics or facts must include a citation or a link to the citation.